
Quality and Quantity Improvement in Healthcare
Project Plan
Project Aim – Reduce late arrivals at clinic appointments in the outpatient department of the hospital by 5% over six months.
Background
This study aims to reduce late appointment attendance at a government hospital in Saudi Arabia. A study shows that 28% of patients arrive late to their outpatient orthopedic clinic appointment in the outpatient department of a government-funded hospital in Saudi Arabia (Nour El-Din et al., 2008). This shows that health care quality is at stake for the same population percentage. Different researchers have studied the major causes of the issues and their implications to the patients and health care organizations. From the studies, a late appointment has been termed a quality problem, especially to the health and safety of the patients (Kasem et al., 2015: Alhamad, 2013). Besides, it has also been linked to economic implications for health care organizations.

- FAST HOMEWORK HELP
- HELP FROM TOP TUTORS
- ZERO PLAGIARISM
- NO AI USED
- SECURE PAYMENT SYSTEM
- PRIVACY GUARANTEED
A late appointment is a quality and safety problem for several reasons based on its impact. Firstly, it negatively impacts patients’ safety and experience. Given that patients’ satisfaction is crucial in determining quality, being late on appointments worsens their experience, compromising the quality of care they receive. For example, if a patient is late for an appointment, the physician is most likely to hurry up while attending to them to cover up the lost time and attend to other scheduled things. This could lead to the physician giving low-quality care because of limited time.
Secondly, it would cause a bottleneck situation, where the hospital experiences a delay in its system. When a delay is caused by late and missed appointments, the entire hospital will be affected. It means that other patients that require other services will also be affected in that there will be limited time to attend to them. Besides, the delay could compromise the system and result in missed appointments. Lastly, it is a quality and safety problem because it could result in financial implications. When patients are late for appointments, physicians have to wait for them, meaning time is lost, which could have been used for other activities that could generate money. If a hospital goes through a financial crisis, the quality of health it offers is affected. Hence, late appointment attendance is a concern that needs to be addressed.
Proposed Intervention
The study aims to reduce late arrivals at clinic appointments in the hospital’s outpatient department by 5% over six months. The rationale for this study is that the issue has dominated many hospitals in Saudi Arabia and other countries in the United Kingdom. This leads to about 1 billion GBP being lost annually (NHS, 2018). Besides, late attendance continues to be witnessed, alarming an action. The rationale was based on a set of causes for late attendance. Some of the causes discovered were; security check time, limited space for parking, a long distance from car parking to the clinic, and limited assistance to get to the clinic. These are the major reasons why the rate of late appointment attendance is high, which has also been verified by several studies (Kasem et al., 2015: Alhamad, 2013). Hence, the study aims to deal with the causes to reduce the rate by 5% over six months.
The method used in the study was the plan–the do–check–act (PDCA) method, where primary drivers were planned, implemented, studied, and adjusted after review. The planning and implementation methods were done within one month each, studied for one week, and acted upon for one month. The method is effective because it allows for the gathering of knowledge for the improvement of a process.
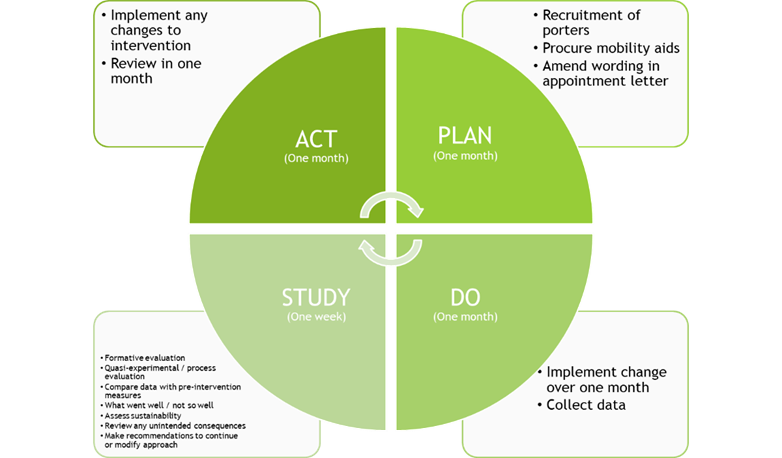
Figure 1: PDCA Cycle
The intervention for reducing late attendances at the clinic involves two main primary drivers. The first one is to assist patients with their mobility. Under this main intervention, there will be three secondary interventions or action steps to take. The first one is to provide porter service from the car park to the clinic for non-mobile patients or those with reduced mobility. This step will be put into action by the human resources team. For example, if a patient has some disabilities, the hospital can help them move from the car parking lot to the clinic through a wheelchair driven by the hospital’s employee. This could help disabled patients stop wasting much time walking to the clinic. As a result, late appointment attendance will be reduced.
The second step of this intervention is to increase mobility aids such as wheelchairs. Not all disabled patients can afford wheelchairs. Hence, making the wheelchairs available at the parking lot to use them would help them minimize walking time from the parking to the clinic. Also, ramps could be put in place to allow patients on wheelchairs to move easier without too many obstacles. The procurement team can implement this intervention since it is concerned with the movement of people and services.

ORDER A CUSTOM ESSAY NOW
HIRE ESSAY TYPERS AND ENJOT EXCELLENT GRADES
Lastly, the intervention can be achieved by altering the improvements on the appointment letter. Even if a hospital provides wheelchairs without informing patients, the provision can be of no benefit. Communication is crucial in every change or quality improvement (Hughes, 2008). The best communication, in this case, is to include the improvement message on the appointment letters so that when patients visit the hospital, they are aware of the facilities that can help them save time. Besides, they will be aware that the hospital is trying to help them save time, hence, take action. The party involved in this intervention is the appointment booking team.
The second primary intervention is improving access to the clinic. After mobilizing the patient, the next thing is to think of the distance to the facility. This intervention involves thinking of an alternative way to enhance clinic access. In this case, the alternative way is to create a drop-off zone near the clinic. For example, the parking can be squeezed near the clinic’s entrance to improve access. To achieve this intervention, three steps need to be taken. Firstly, the appointment letters need to be altered and include a drop-off zone being created near the clinic. The purpose is to inform patients so that they know that they can access the clinic more conveniently.
The second step is to add signage at the parking lot to show people where the new drop-off zone is. This is also a communication strategy that will see patients taking action. For example, instead of dropping off a patient at the previous lot, the patient can be dropped at the new drop-off zone to save time. The estates’ team of a hospital can do this. The justification for the two interventions is that they will help save patients’ time, and consequently, patients will be on time, reducing late appointment attendances. For example, in the first intervention, assisting patients with their mobility use of wheelchairs will definitely save them time. Also, making the clinic more accessible will help reduce patients’ time looking for it and walking from the parking lot. In the end, a reduced late attendance for appointments will be witnessed.
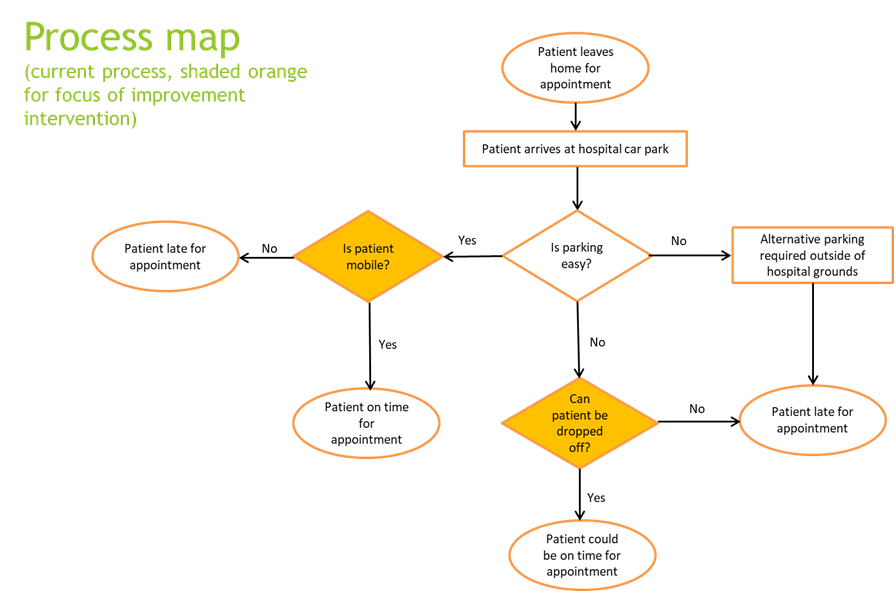
Figure 2: Process map
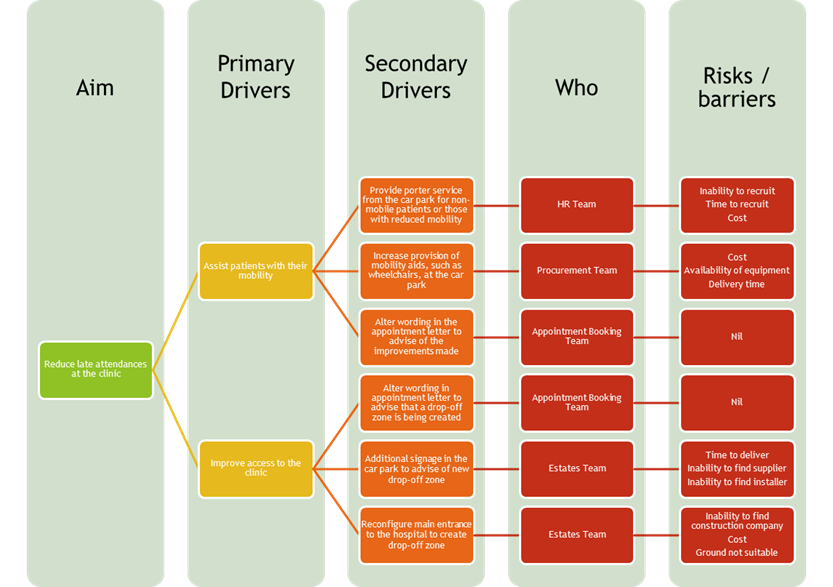
Figure 3: Drivers to successful implementation
Improvement will be measured after the specified six months using four parameters. The parameters include; productivity and efficiency, patient experience, staff experience, and cost incurred. The productivity and efficiency parameters will be measured in terms of the number of patients arriving on time, feedback from staff, and clinic productivity using time and motion. Several overall changes will signify improvement. The first one is when appointment slots increase, and bottlenecking is reduced. Secondly, when patients have to wait for a short time, their satisfaction increases. Thirdly, when staff is motivated to work, their work satisfaction is improved. Lastly, unnecessary costs will be reduced, such as overtime pay due to staff working late hours and clinic costs due to unplanned hours.
Critique and reflection
The major critique centers on how scholars and researchers assume that late appointment attendance negatively affects patients’ experience and satisfaction and affects their quality and safety. According to a study, patients who arrive late for appointments are more satisfied than those who arrive on time or earlier (Medway et al., 2016). I find this making sense because they arrive late, wait for a shorter time, or just go straight to the doctor. This minimizes their waiting time, making them more satisfied with getting straight services without having to wait. On the other hand, those who arrive earlier wait for a longer time, which probably worsens their experiences and reduces their satisfaction.

Therefore, as much as the study terms late appointment attendances a quality and safety problem, it is not. There is no ground evidence to show that patients who arrive earlier or on time for appointments get quality services than those who arrive late. I feel that a doctor will always give quality services to all patients regardless of whether they come early or late. The point is that as long as the patient and the doctor have met, the services remain the same. Besides, as the study revealed, those who arrive late have the worst patient experience because they have to wait long before being attended on.
In conclusion, despite the critiques, the benefits of reduced late appointment attendances are beyond measure for both patients and hospitals. However, the interventions should be implemented while also considering the implications of patients arriving too early.